
CHAPTER 6 : ECG LEADS AND MONITER LEADS
2 posters
Page 1 of 1

CHAPTER 6 : ECG LEADS AND MONITER LEADS
![]() by Admin Tue Mar 16 2010, 01:19
by Admin Tue Mar 16 2010, 01:19
Chest (Precordial) Leads
The chest leads (V1 to V6 ) show the electrical currents of
the heart as detected by electrodes placed at different positions on the chest
wall. The precordial leads used today are also unipolar leads in that they
measure the voltage in any one location relative to zero potential. The chest
leads are recorded simply by means of electrodes (usually attached to suction
cups to hold them in place on the chest) at six designated locations on the
chest wall . Two points are worth mentioning here:
1.
The fourth intercostal space can be located by
placing your finger at the top of the sternum and moving it slowly downward.
After you move your finger down about 11 /2 inches, you can feel a slight horizontal
ridge. This is called the angle of Louis, which is located where the manubrium
joins the body of the sternum. The second intercostal space is just below and
lateral to this point. Move down two more spaces. You are now in the fourth
interspace and ready to place lead V4 .
2.
Chest lead placement in females is complicated
by breast tissue, which may result in misplacement of the chest leads. In
taking ECGs on women, you must remember to place the electrode under the breast
for leads V3 to V6 . If, as often happens, the electrode is placed on the
breast, electrical voltages from higher interspaces are recorded. Also, never
use the nipples to locate the position of any of the chest lead electrodes,
even in men, because nipple location varies greatly in different persons.

Like the other leads, each chest lead has a positive and
negative pole. The positive pole of each chest lead points anteriorly, toward
the front of the chest. The negative pole of each chest lead points
posteriorly, toward the back.
The 12-Lead ECG: Frontal and Horizontal Plane Leads:
The importance of multiple leads is illustrated in the
diagnosis of myocardial infarction (MI). An MI typically affects one localized
portion of either the anterior or inferior portion of the left ventricle. The
ECG changes produced by an anterior MI are usually best shown by the chest
leads, which are close to and face the injured anterior surface of the heart.
The changes seen with an inferior MI usually appear only in leads such as II,
III, and aVf , which face the injured inferior surface of the heart . The 12
leads therefore provide a three-dimensional view of the electrical activity of
the heart.

Specifically, the six extremity leads (I, II, III, aVr , aVl
, aVf ) record electrical voltages transmitted onto the frontal plane of the
body. (In contrast, the six precordial leads record voltages transmitted onto
the horizontal plane.) For example, if you walk up to and face a large window,
the window is parallel to the frontal plane of your body. Similarly, heart
voltages directed upward and downward and to the right and left are recorded by
the frontal plane leads.
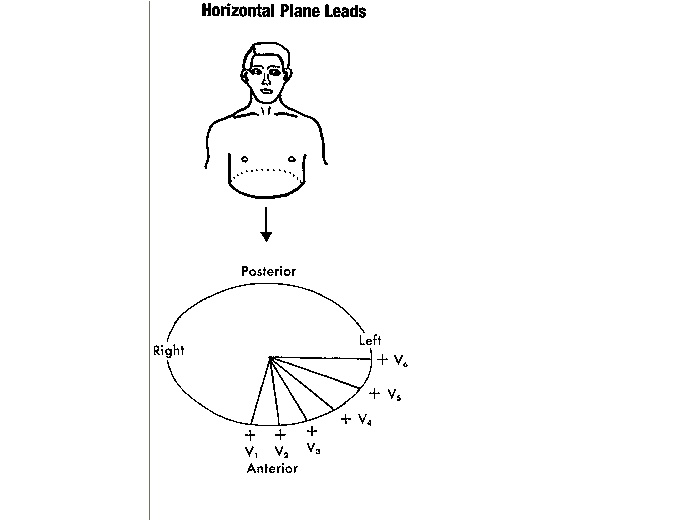
The six chest leads (V1 through V6 ) record heart voltages
transmitted onto the horizontal plane of the body . The horizontal plane cuts
your body into an upper and a lower half. Similarly, the chest leads record
heart voltages directed anteriorly (front) and posteriorly (back), and to the
right and left.
Cardiac Monitors and Monitor Leads
BEDSIDE CARDIAC MONITORS
Up to now, only the standard 12-lead ECG has been
considered. However, it is not always necessary or feasible to record a full
12-lead ECG. For example, many patients require continuous monitoring for a
prolonged period. In such cases, special cardiac monitors are used to give a
continuous beat-to-beat record of cardiac activity from one monitor lead.
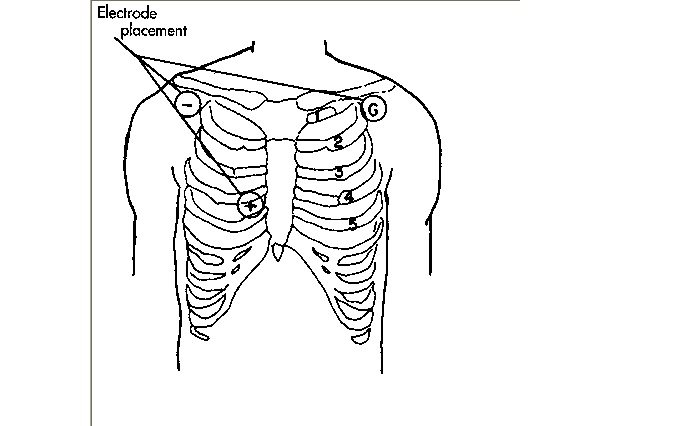
Below is a rhythm strip recorded from a monitor lead
obtained by means of three disk electrodes on the chest wall. The electrodes
for recording the strip is kept as shown in the figure below, one electrode
(the positive one) is usually pasted in the V1 position. The other two are
placed near the right and left shoulders. One serves as the negative electrode
and the other as the ground.

When the location of the electrodes on the chest wall is
varied, the resultant ECG patterns also vary. In addition, if the polarity of
the electrodes changes (e.g., the negative electrode is connected to the V1
position and the positive electrode to the right shoulder), the ECG shows a
completely opposite pattern.
AMBULATORY MONITORS
The cardiac monitors just described are useful in patients confined
to a bed or chair. Sometimes, however, heartbeat needs to be recorded in
ambulatory patients over longer periods. A special portable ECG system,
designed in 1961 by N.J. Holter, records the cardiac activity of patients as
they go about their daily activities.
The Holter monitor currently in use consists of electrodes
placed on the chest wall and lower abdomen and a special portable ECG recorder.
The patient can then be monitored over a long period (e.g., 24 hours). Two ECG
leads are usually recorded. The tape is played back, and the P-QRS-T complexes
are displayed on a special screen. Printouts of any portion of the ECG can be
obtained for further study and permanent records.
Portable patient-activated monitors are now available to
record ECGs in individuals with very intermittent symptoms. These event
recorders are designed with replaceable electrodes so that patients can be
monitored for several weeks as they go about their usual activities.
The chest leads (V1 to V6 ) show the electrical currents of
the heart as detected by electrodes placed at different positions on the chest
wall. The precordial leads used today are also unipolar leads in that they
measure the voltage in any one location relative to zero potential. The chest
leads are recorded simply by means of electrodes (usually attached to suction
cups to hold them in place on the chest) at six designated locations on the
chest wall . Two points are worth mentioning here:
1.
The fourth intercostal space can be located by
placing your finger at the top of the sternum and moving it slowly downward.
After you move your finger down about 11 /2 inches, you can feel a slight horizontal
ridge. This is called the angle of Louis, which is located where the manubrium
joins the body of the sternum. The second intercostal space is just below and
lateral to this point. Move down two more spaces. You are now in the fourth
interspace and ready to place lead V4 .
2.
Chest lead placement in females is complicated
by breast tissue, which may result in misplacement of the chest leads. In
taking ECGs on women, you must remember to place the electrode under the breast
for leads V3 to V6 . If, as often happens, the electrode is placed on the
breast, electrical voltages from higher interspaces are recorded. Also, never
use the nipples to locate the position of any of the chest lead electrodes,
even in men, because nipple location varies greatly in different persons.
| Conventional Placement of ECG Chest Leads Lead V1 is recorded with the electrode in the fourth intercostal space just to the right of the sternum. Lead V2 is recorded with the electrode in the fourth intercostal space just to the left of the sternum. Lead V3 is recorded on a line midway between leads V2 and V4 . Lead V4 is recorded in the midclavicular line in the fifth interspace. Lead V5 is recorded in the anterior axillary line at the same level as lead V4 . Lead V6 is recorded in the midaxillary line at the same level as lead V4 . |
Like the other leads, each chest lead has a positive and
negative pole. The positive pole of each chest lead points anteriorly, toward
the front of the chest. The negative pole of each chest lead points
posteriorly, toward the back.
The 12-Lead ECG: Frontal and Horizontal Plane Leads:
The importance of multiple leads is illustrated in the
diagnosis of myocardial infarction (MI). An MI typically affects one localized
portion of either the anterior or inferior portion of the left ventricle. The
ECG changes produced by an anterior MI are usually best shown by the chest
leads, which are close to and face the injured anterior surface of the heart.
The changes seen with an inferior MI usually appear only in leads such as II,
III, and aVf , which face the injured inferior surface of the heart . The 12
leads therefore provide a three-dimensional view of the electrical activity of
the heart.
Specifically, the six extremity leads (I, II, III, aVr , aVl
, aVf ) record electrical voltages transmitted onto the frontal plane of the
body. (In contrast, the six precordial leads record voltages transmitted onto
the horizontal plane.) For example, if you walk up to and face a large window,
the window is parallel to the frontal plane of your body. Similarly, heart
voltages directed upward and downward and to the right and left are recorded by
the frontal plane leads.
The six chest leads (V1 through V6 ) record heart voltages
transmitted onto the horizontal plane of the body . The horizontal plane cuts
your body into an upper and a lower half. Similarly, the chest leads record
heart voltages directed anteriorly (front) and posteriorly (back), and to the
right and left.
Cardiac Monitors and Monitor Leads
BEDSIDE CARDIAC MONITORS
Up to now, only the standard 12-lead ECG has been
considered. However, it is not always necessary or feasible to record a full
12-lead ECG. For example, many patients require continuous monitoring for a
prolonged period. In such cases, special cardiac monitors are used to give a
continuous beat-to-beat record of cardiac activity from one monitor lead.
Below is a rhythm strip recorded from a monitor lead
obtained by means of three disk electrodes on the chest wall. The electrodes
for recording the strip is kept as shown in the figure below, one electrode
(the positive one) is usually pasted in the V1 position. The other two are
placed near the right and left shoulders. One serves as the negative electrode
and the other as the ground.
When the location of the electrodes on the chest wall is
varied, the resultant ECG patterns also vary. In addition, if the polarity of
the electrodes changes (e.g., the negative electrode is connected to the V1
position and the positive electrode to the right shoulder), the ECG shows a
completely opposite pattern.
AMBULATORY MONITORS
The cardiac monitors just described are useful in patients confined
to a bed or chair. Sometimes, however, heartbeat needs to be recorded in
ambulatory patients over longer periods. A special portable ECG system,
designed in 1961 by N.J. Holter, records the cardiac activity of patients as
they go about their daily activities.
The Holter monitor currently in use consists of electrodes
placed on the chest wall and lower abdomen and a special portable ECG recorder.
The patient can then be monitored over a long period (e.g., 24 hours). Two ECG
leads are usually recorded. The tape is played back, and the P-QRS-T complexes
are displayed on a special screen. Printouts of any portion of the ECG can be
obtained for further study and permanent records.
Portable patient-activated monitors are now available to
record ECGs in individuals with very intermittent symptoms. These event
recorders are designed with replaceable electrodes so that patients can be
monitored for several weeks as they go about their usual activities.

Admin- Admin
- Posts : 76
Reputation : 8
Join date : 2010-01-06
Age : 34
Location : chennai
Re: CHAPTER 6 : ECG LEADS AND MONITER LEADS
![]() by Admin Tue Mar 16 2010, 01:23
by Admin Tue Mar 16 2010, 01:23
Questions
1.Leads I and II are shown below. Draw the P-QRS-T pattern
in lead III.

2.Leads I, II, and III are shown below. What is wrong with
them?

1.Leads I and II are shown below. Draw the P-QRS-T pattern
in lead III.
2.Leads I, II, and III are shown below. What is wrong with
them?
Admin- Admin
- Posts : 76
Reputation : 8
Join date : 2010-01-06
Age : 34
Location : chennai
Re: CHAPTER 6 : ECG LEADS AND MONITER LEADS
![]() by gogeta Wed Mar 24 2010, 21:53
by gogeta Wed Mar 24 2010, 21:53
here 1 + 2 is equal to 3 da
they are wrongly named !
they are wrongly named !
gogeta- NeWBie

- Posts : 17
Reputation : 0
Join date : 2010-01-13
» CHAPTER 5 : ECG LEADS
» CHAPTER 2 : Basic waves
» CHAPTER 3 : Basic waves part 2
» CHAPTER 4 : BASIC WAVES , HEART RATE
» CHAPTER 7 : NORMAL WAVES "P"
» CHAPTER 2 : Basic waves
» CHAPTER 3 : Basic waves part 2
» CHAPTER 4 : BASIC WAVES , HEART RATE
» CHAPTER 7 : NORMAL WAVES "P"
Page 1 of 1
Permissions in this forum:
You cannot reply to topics in this forum